10th International Congress on Ambulatory Surgery.
A. Jiménez, J.A. Gracia, E. Redondo, B. Calvo, B. Jiménez, M. Martínez.

BACKGROUND.

Day surgery is expanding quickly in Spain and Spanish Hospitals are reaching an ambulatorization index (percentage of interventions performed in day surgery by all specialties) near 50%. As well as studying the outcomes of surgery it is also important to look at the “customer satisfaction” of a given service. Following the recommendation of Rudkin, patient satisfaction surveys must be performed in order to obtain comments from dissatisfied patients, explore the reasons for them and thus improve the quality of care.
The Day Surgery Unit (DSU) of U.H. Lozano Blesa in Zaragoza-Spain began its activity in 1995. In April 1999 a questionnaire, designed by experts, was implemented in the hospital in order to know the patient satisfaction in ambulatory surgery.

From that time until today there have been important changes in the unit. Protocols of postoperative pain control were improved in year 2000. In year 2009, some beds in the recovery area were replaced by recliner chairs increasing the number of patient cubicles from 12 to 17 with an important increase in outpatient surgery. Finally last year, forced by the financial and economic crisis in Europe, the activity in ambulatory surgery stopped its progression due to budget cuts imposed by the European Union to Spain provoking an important increase of number of patients in waiting lists.
OBJECTIVE.

Our aim is to analyze information provided by questionnaires in order to identify complaints, areas of improvement, the effects provoked by the increase of activity and, nowadays, the effects of budget cuts.
METHODS.

Our study has been done in a multidisciplinary DSU, integrated in a University General Hospital with independent facilities. Patients belonged to Ophthalmology, General Surgery and Orthopedic Surgery principally.

An anonymous questionnaire to be returned in a prepaid envelope, with 25 scaled close-ended items and 6 demographic variables, was delivered to 21631 patients, operated on in our day surgery unit from April 1999 to November
2012, at the moment of discharge. Questions were grouped in 5 different areas: 1. Patient information and contact, 2. Patient comfort, 3. Health care provided, 4. Hospitality and organization, 5. General satisfaction. The answers were transformed into a score system with a maximum of 20 points per area and 100 points per questionnaire. The recommendation was to fill in the questionnaire one or two weeks after surgery and return it by mail.

Answers and scores were registered in a database created with Stat-View 5.1.0 software. This program allows descriptive statistics and comparisons. Statistical comparisons were made with ANOVA test. Significance was defined as p<0 .05.="">


A 84 per cent of responders were satisfied with day surgery unit and 95 per cent would choose the unit again if necessary. The average total score was 84,6 and only 19 questionnaires had the total score below 50. The fluctuation of this score was statistically significant during these years with the worst data at the beginning of DSU activity and in the years 2010 and 2011 in which there was an important increase of activity.


- Area number 1 (Patient information and contact): 17.7 points (maximum 20). Responders were satisfied with the information about day surgery and the possibility of phone contact 24 hours. Only the question about preoperative information reflects improvement possibilities. The score on this preoperative information did not suffer significant variations during the studied years.




- Area number 3 (Health care provided): 16.2 points (maximum 20). Patients were very satisfied with health cares provided at the DSU but the large waiting list impairs the score of this area. Analysing variations of waiting list score we have discovered an important statistical significance during these years, with the worst data in year 2012 coinciding with the budget cuts and the increased list.



- Area number 5 (General Satisfaction): 17.1 points (maximum 20). Satisfaction was very high in this area but responders said that health workers asked for their opinion about cares rarely. Although cares at the DSU are protocolized, nurses and physicians should give further explanations to patients about the cares provided in the unit. The patients’ complaint about the possibility to discuss cares with health workers has remained stable during these years.


The demographic variables allowed comparisons among patients finding statistical significance. The highest scores were associated with male patients, with the age between 41 and 65 years, married and with the higher level of education. The lowest scores were associated with female patients, with age under 40 years, widowers and the primary level of education. There were no statistical differences related to rural/urban habitat or employment.

CONCLUSIONS.
REFERENCES.
-A. Jiménez et al. Encuesta de satisfacción en cirugía mayor ambulatoria: Instrumentos para detectar puntos débiles y monitorizar mejoras. Cir May Amb 2002; 7(4):164-172
-P. Lemos et al. Patient satisfaction following day surgery. J Clin Anesth 2009; 21(3):200-5
-S. Mcintosh and J Adams. Anxiety and quality of recovery in day surgery: A questionnaire study using Hospital Anxiety and Depression Scale and Quality of Recovery Score. Int J Nurs Pract 2011; 17(1):85-92
- I. Shnaider and F. Chung. Outcomes in day surgery. Curr OIpin Anaesthesiol 2006; 19(6): 622-9.
-MW. Stomberg et al. Day surgery, variations in routines and practices a questionnaire survey. Int J Surg. 2013; Jan 9. Pii:S1743-9191 (13)
-D. Tong et al. Predictive factors in global and anesthesia satisfaction in ambulatory surgical patients. Anesthesiology 1997; 87:856-64
RESULTS.


A total of 9283 patients (43 per cent) responded. The demographic characteristics of responders were: Gender: 50.6 per cent were men and 47 per cent women. Age: mean age was 59 years with a median of 62 years. Habitat: 65 per cent lived in urban environment and 32 per cent in rural areas. Civil status: 67 per cent were married, 14 per cent were single and 13 widowed. Level of education: 52 per cent had primary education, 23 per cent had secondary education and 11 per cent were graduates. Employment: 33 per cent were employed, 40 per cent retired, 4 per cent unemployed and 18 per cent were housewives.

A 84 per cent of responders were satisfied with day surgery unit and 95 per cent would choose the unit again if necessary. The average total score was 84,6 and only 19 questionnaires had the total score below 50. The fluctuation of this score was statistically significant during these years with the worst data at the beginning of DSU activity and in the years 2010 and 2011 in which there was an important increase of activity.

The analysis of areas showed:


- Area number 1 (Patient information and contact): 17.7 points (maximum 20). Responders were satisfied with the information about day surgery and the possibility of phone contact 24 hours. Only the question about preoperative information reflects improvement possibilities. The score on this preoperative information did not suffer significant variations during the studied years.

- Area number 2 (Patient comfort): 15.1 points (maximum 20). Anxiety during the night before surgery and deficiencies in the postoperative pain control were detected. Both findings should force a change in protocols to improve the control of preoperative anxiety and postoperative pain. Analysing the behaviour of the anxiety before surgery and postoperative pain scores during these years we found no significant differences.
- Area number 3 (Health care provided): 16.2 points (maximum 20). Patients were very satisfied with health cares provided at the DSU but the large waiting list impairs the score of this area. Analysing variations of waiting list score we have discovered an important statistical significance during these years, with the worst data in year 2012 coinciding with the budget cuts and the increased list.
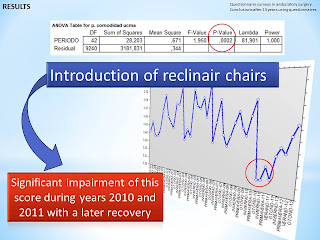
- Area number 4 (Hospitality and organization): 18.5 points (maximum 20). Patients were very satisfied with the five questions of this area. However, it was important to know if the introduction of 9 recliner chairs in 2009 has impaired the specific score about comfort in the recovery area. The line plot shows a significant impairment of this score during 2010 and 2011 with a later recovery.
- Area number 5 (General Satisfaction): 17.1 points (maximum 20). Satisfaction was very high in this area but responders said that health workers asked for their opinion about cares rarely. Although cares at the DSU are protocolized, nurses and physicians should give further explanations to patients about the cares provided in the unit. The patients’ complaint about the possibility to discuss cares with health workers has remained stable during these years.
The demographic variables allowed comparisons among patients finding statistical significance. The highest scores were associated with male patients, with the age between 41 and 65 years, married and with the higher level of education. The lowest scores were associated with female patients, with age under 40 years, widowers and the primary level of education. There were no statistical differences related to rural/urban habitat or employment.

CONCLUSIONS.
1. Questionnaire surveys in ambulatory surgery allow, not only to know patients satisfaction, but to identify the reasons for patients dissatisfaction.
2. The transformation of qualitative data in a score system allows to monitor improvements and to compare groups of patients by applying more powerful statistical tests.
3. The most important area of improvement is related to waiting lists but there are also necessary actions in order to improve preoperative information, reduce anxiety the night before surgery, relief postoperative pain and to give more explanations about cares to patients.
2. The transformation of qualitative data in a score system allows to monitor improvements and to compare groups of patients by applying more powerful statistical tests.
3. The most important area of improvement is related to waiting lists but there are also necessary actions in order to improve preoperative information, reduce anxiety the night before surgery, relief postoperative pain and to give more explanations about cares to patients.
REFERENCES.
-S. Ghosh and S. Sallam. Patient satisfaction and postoperative demands on hospital and community services after day surgery. Br J Surg 1994; 81:1635-1638
-A. Jiménez et al. Encuesta de satisfacción en cirugía mayor ambulatoria: Instrumentos para detectar puntos débiles y monitorizar mejoras. Cir May Amb 2002; 7(4):164-172
-P. Lemos et al. Patient satisfaction following day surgery. J Clin Anesth 2009; 21(3):200-5
-S. Mcintosh and J Adams. Anxiety and quality of recovery in day surgery: A questionnaire study using Hospital Anxiety and Depression Scale and Quality of Recovery Score. Int J Nurs Pract 2011; 17(1):85-92
- I. Shnaider and F. Chung. Outcomes in day surgery. Curr OIpin Anaesthesiol 2006; 19(6): 622-9.
-MW. Stomberg et al. Day surgery, variations in routines and practices a questionnaire survey. Int J Surg. 2013; Jan 9. Pii:S1743-9191 (13)
-D. Tong et al. Predictive factors in global and anesthesia satisfaction in ambulatory surgical patients. Anesthesiology 1997; 87:856-64
Your informational post is great resource to lots of peoples, so i would like to thank for creating this interesting blog.
ResponderEliminar